import { virusInfoOrUndefinedF } from "/_js/functions.js"
import { availableVirusInfoF } from "/_js/functions.js"
import { availableToolsF } from "/_js/functions.js"
import { virusOfInterestF } from "/_js/functions.js"
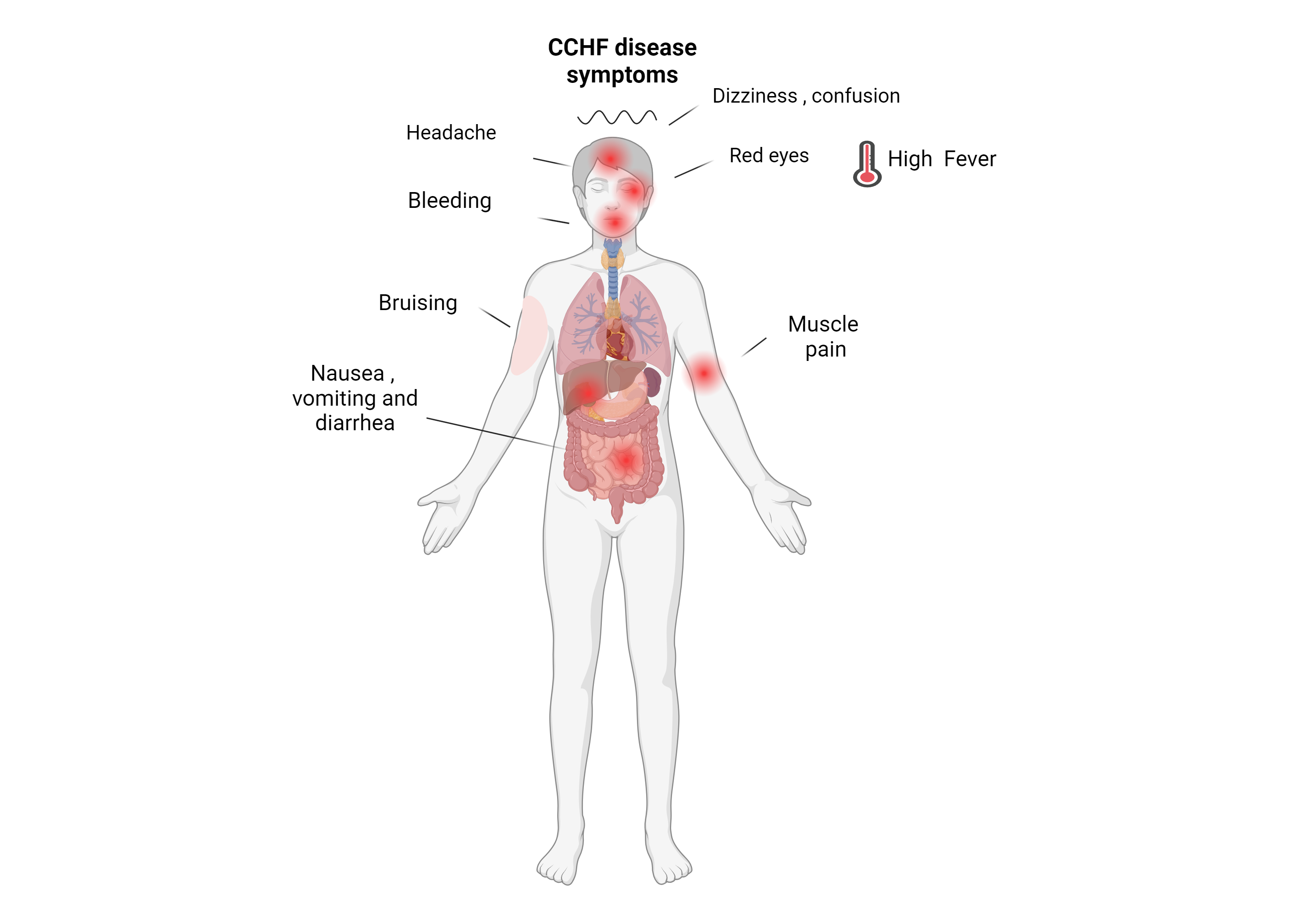
Hemorrhagic phase progression with bruising, nosebleeds, and bleeding at injection sites can be seen. Beginning 4 days after illness and lasting for about two weeks.
Other clinical signs include: tachycardia, lymphadenopathy, and a petechiae (a rash caused by bleeding into the skin) on internal mucosal surfaces, such as in the mouth and throat, and on the skin. Hepatitis, and severely ill patients may experience rapid kidney deterioration, liver failure or pulmonary failure after 5 days of illness.
![]()
The virus was first observed in Crimea in the 1940s and was later identified as the same agent of what had been called Congo Hemorrhagic Fever.
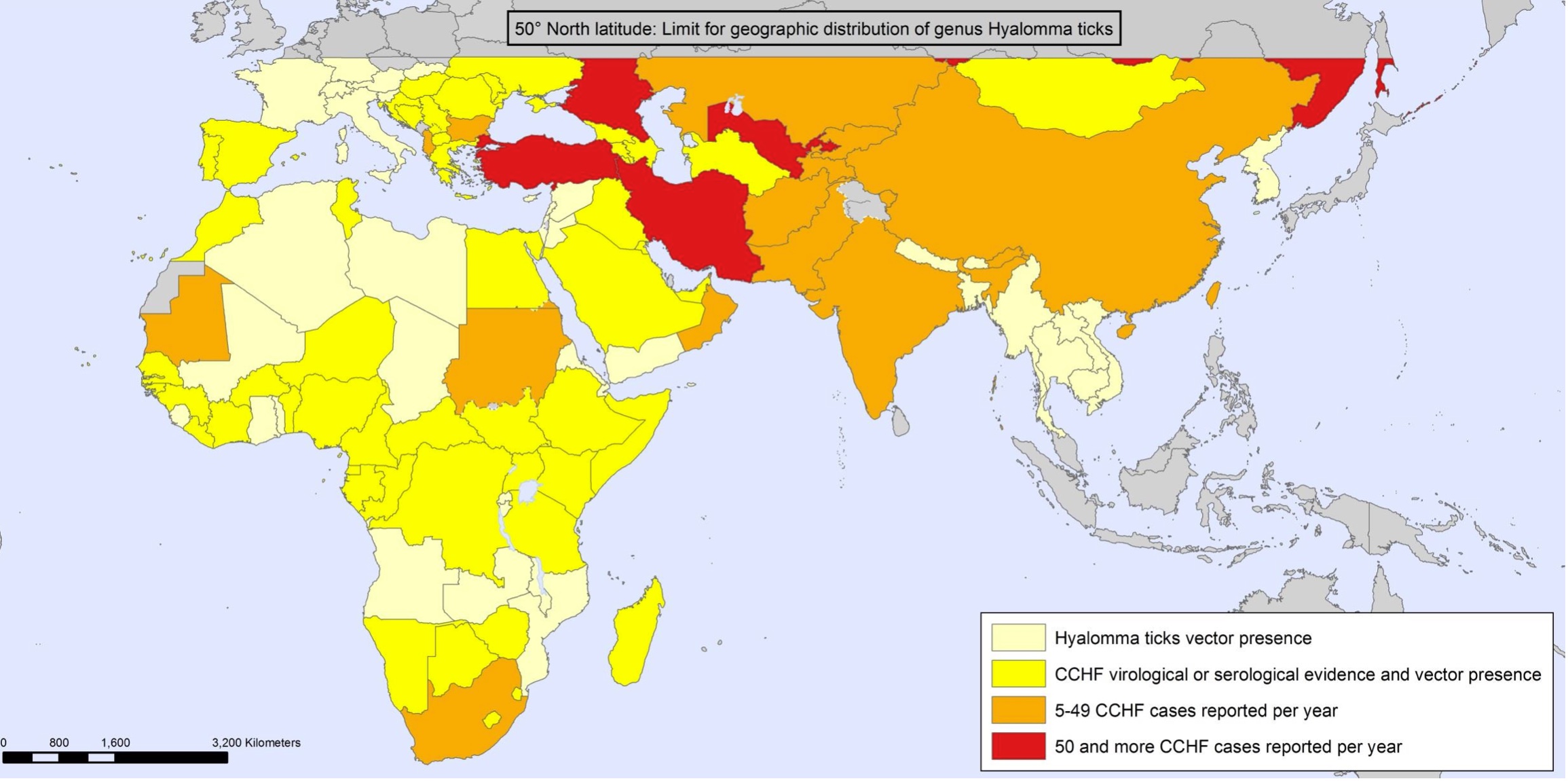
CCHFV is among the most widely distributed hemorrhagic fever viruses with cases reported through Africa, the Middle East, Asia, and Southern and Eastern Europe.
The fatality rate is typically between 10 and 40%, though fatalities as high as 80% have been observed in some outbreaks.
CCHF is on WHO’s priority list for Research and Development and the US National Institute of Allergy and Infectious Diseases (NIH/NIAID) priority A list, as a disease posing the highest level of risk to national security and public health.
The toolbox for this virus is currently in development. Please contact us via info@virusbankplatform.be for more information.
![]()
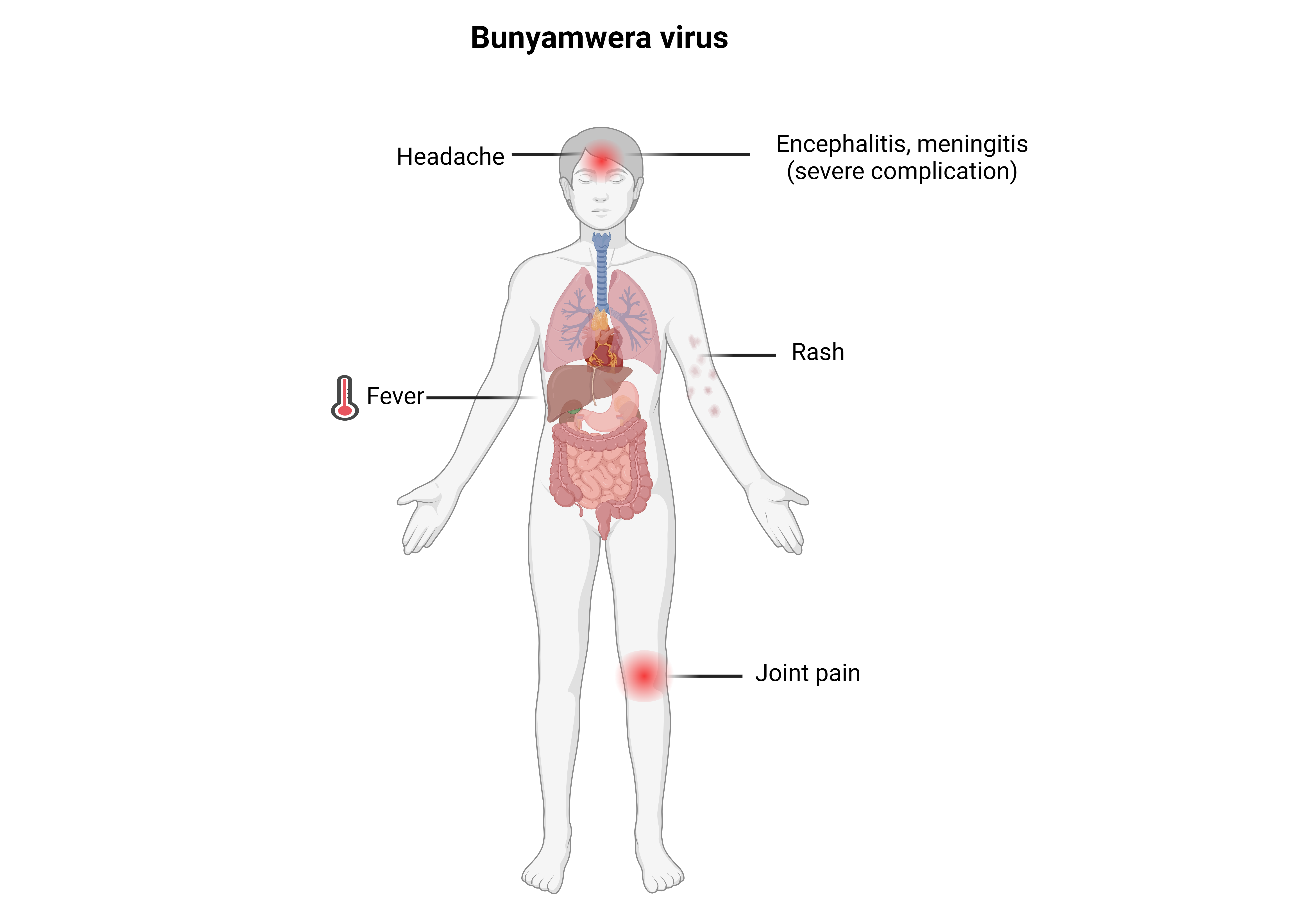
It is named for Bunyamwera, a town in western Uganda, where it was isolated in 1943.
In endemic areas such as sub-Saharan Africa, seroprevalence has been recorded as high as 82% in some areas.
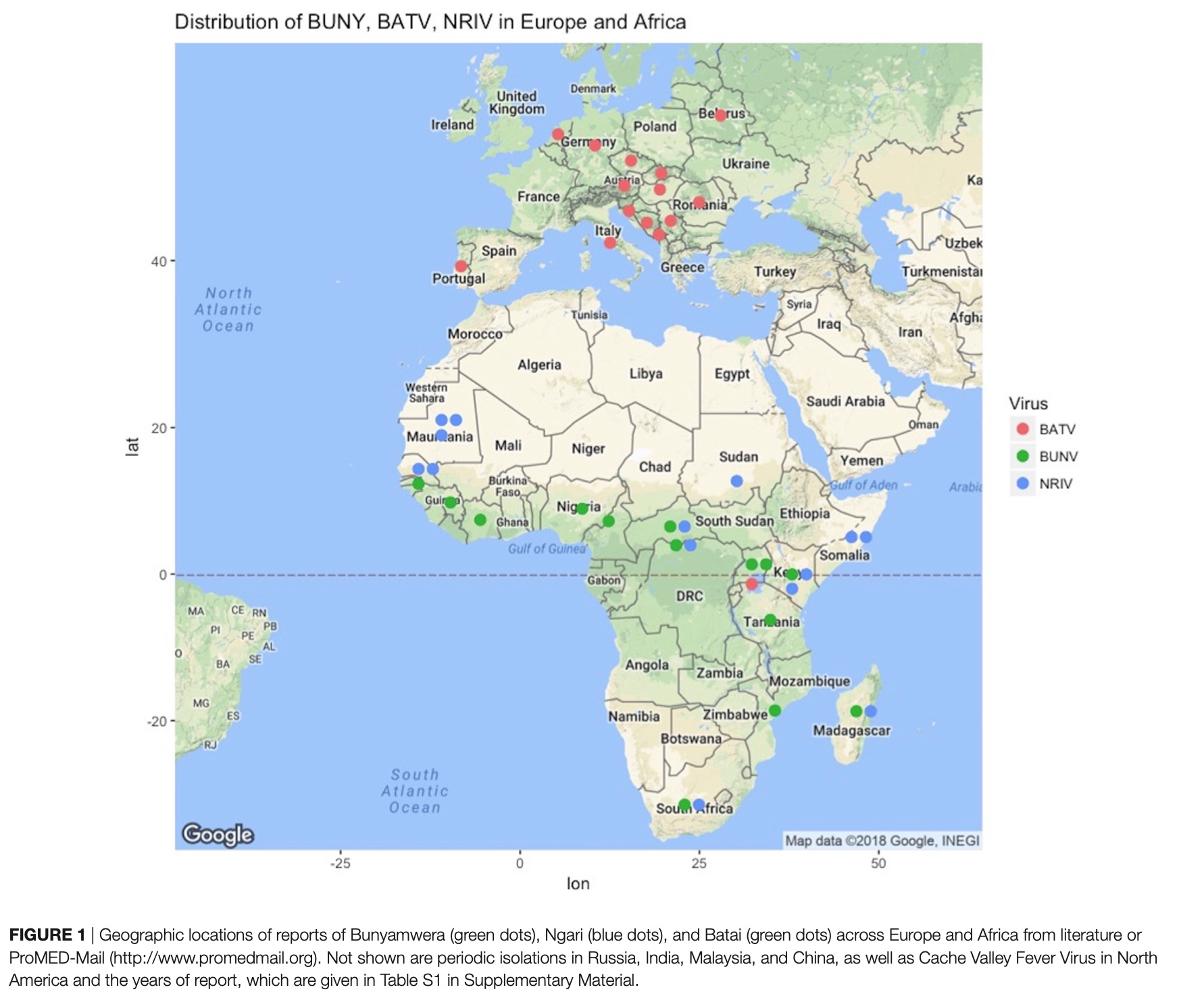
Bunyamwera virus (BUNV) is present on both the African and South American continents.
The toolbox for this virus is currently in development. Please contact us via info@virusbankplatform.be for more information.
![]()
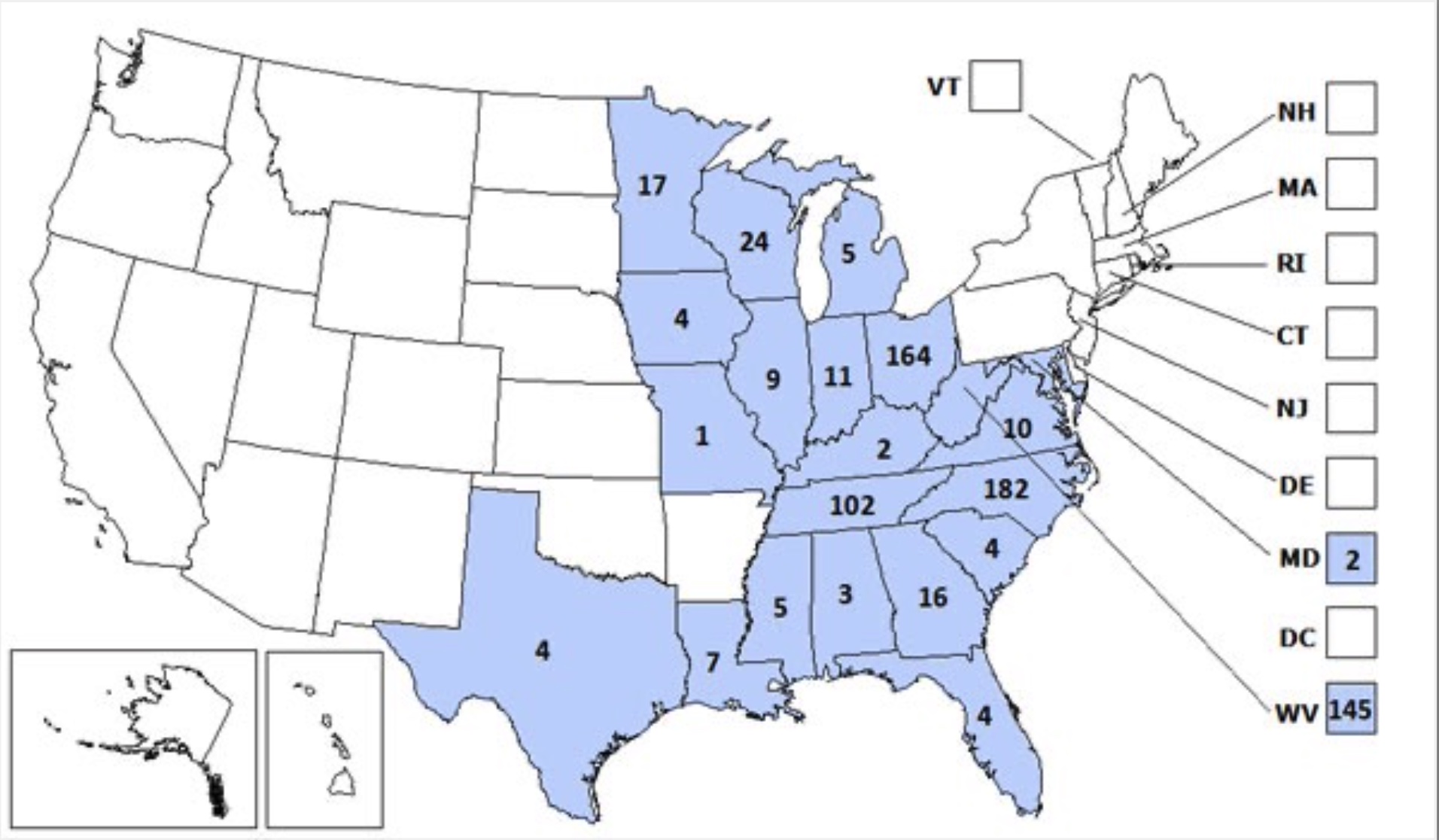
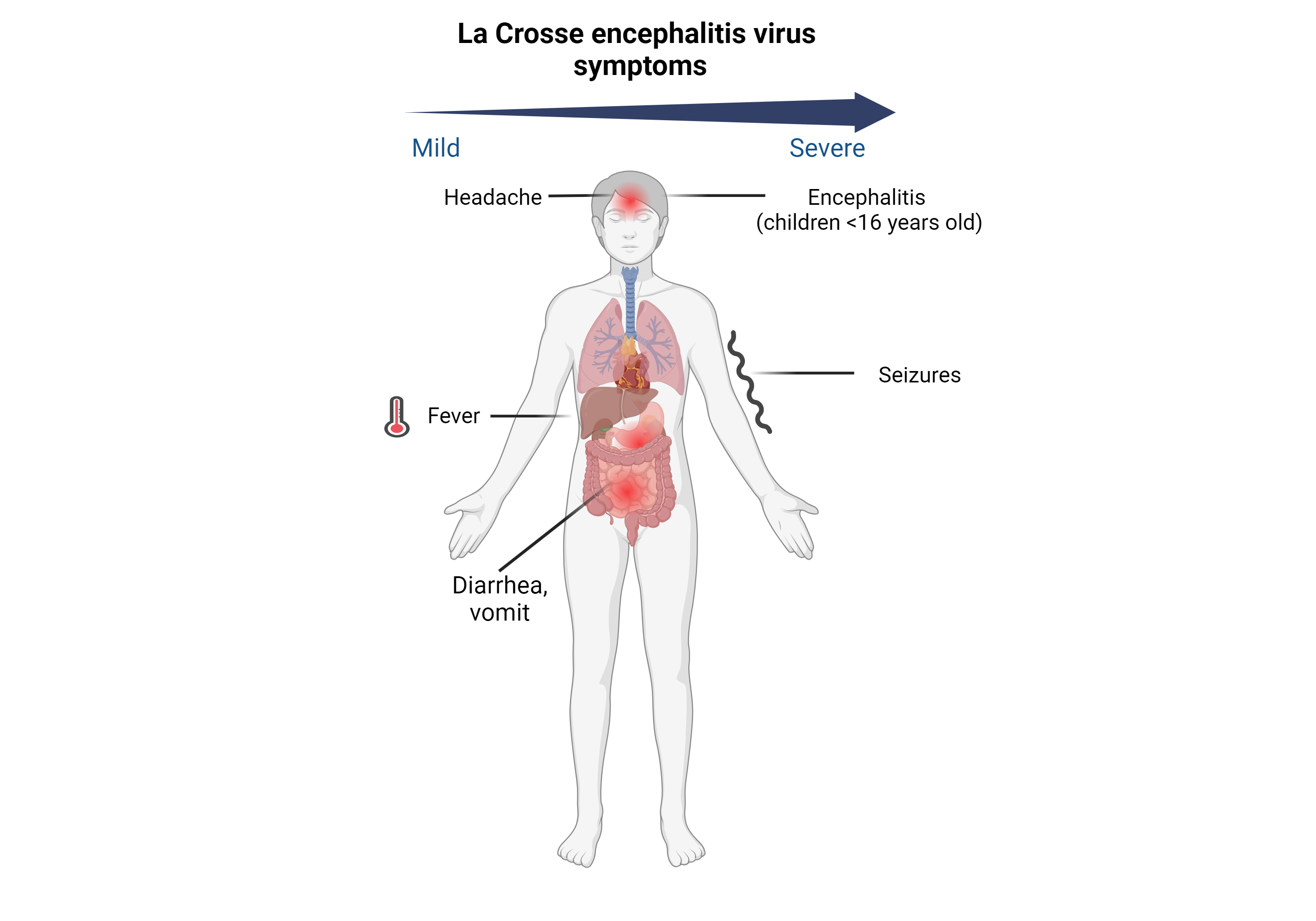
In the United States, about 80–100 LACV disease cases are reported each year, although it is believed to be under-reported due to minimal symptoms experienced by many of those affected.
LAC encephalitis is rare. Death from LAC encephalitis occurs in less than 1% of clinical cases
The toolbox for this virus is currently in development. Please contact us via info@virusbankplatform.be for more information.
![]()
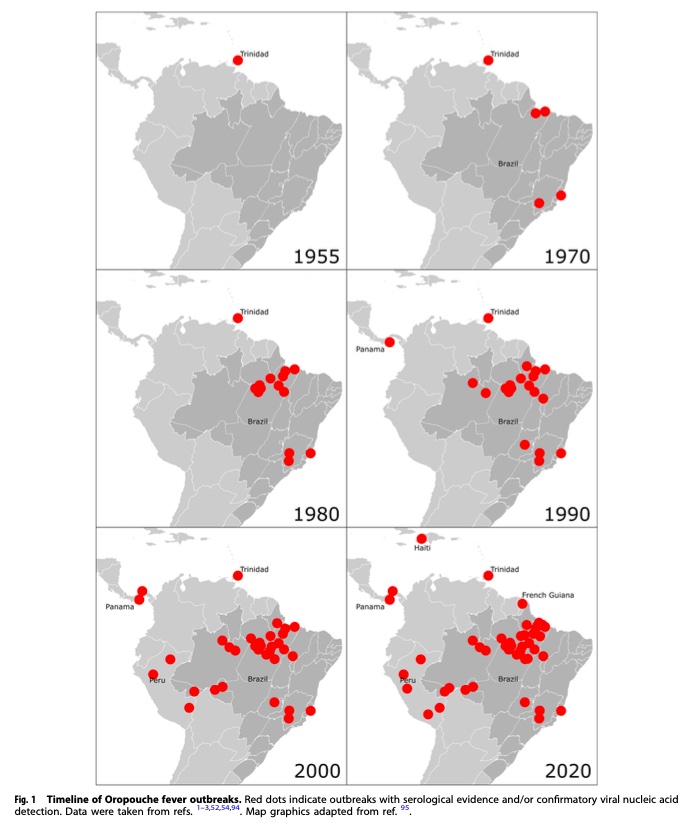
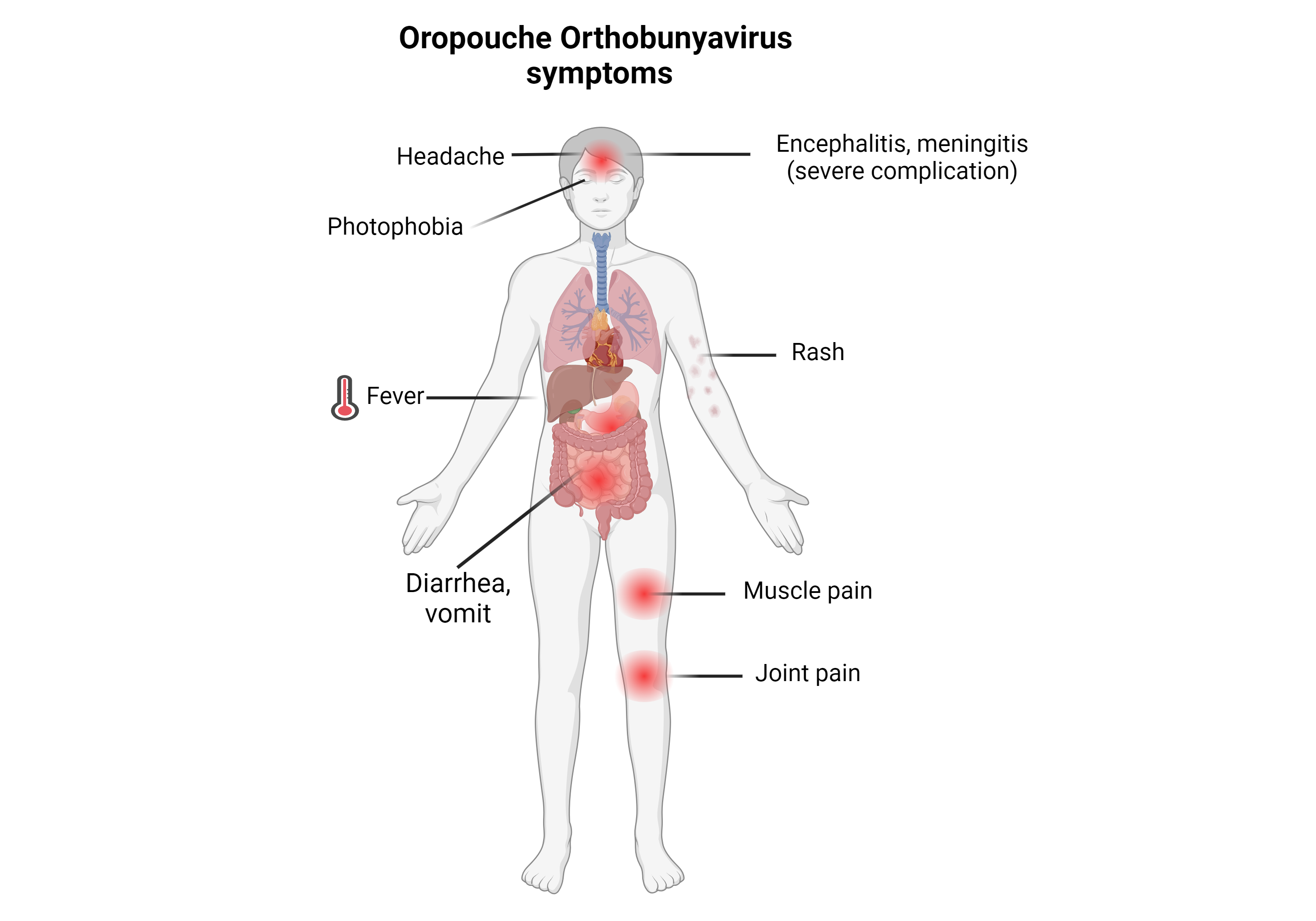
This disease is named after the region where it was first discovered and isolated at the Trinidad Regional Virus Laboratory in 1955 by the Oropouche River in Trinidad and Tobago.
The virus is considered a public health threat in tropical and subtropical areas of Central and South America, with over half a million infected people as of 2005. >30 epidemics during 1960–2009.
The toolbox for this virus is currently in development. Please contact us via info@virusbankplatform.be for more information.
![]()
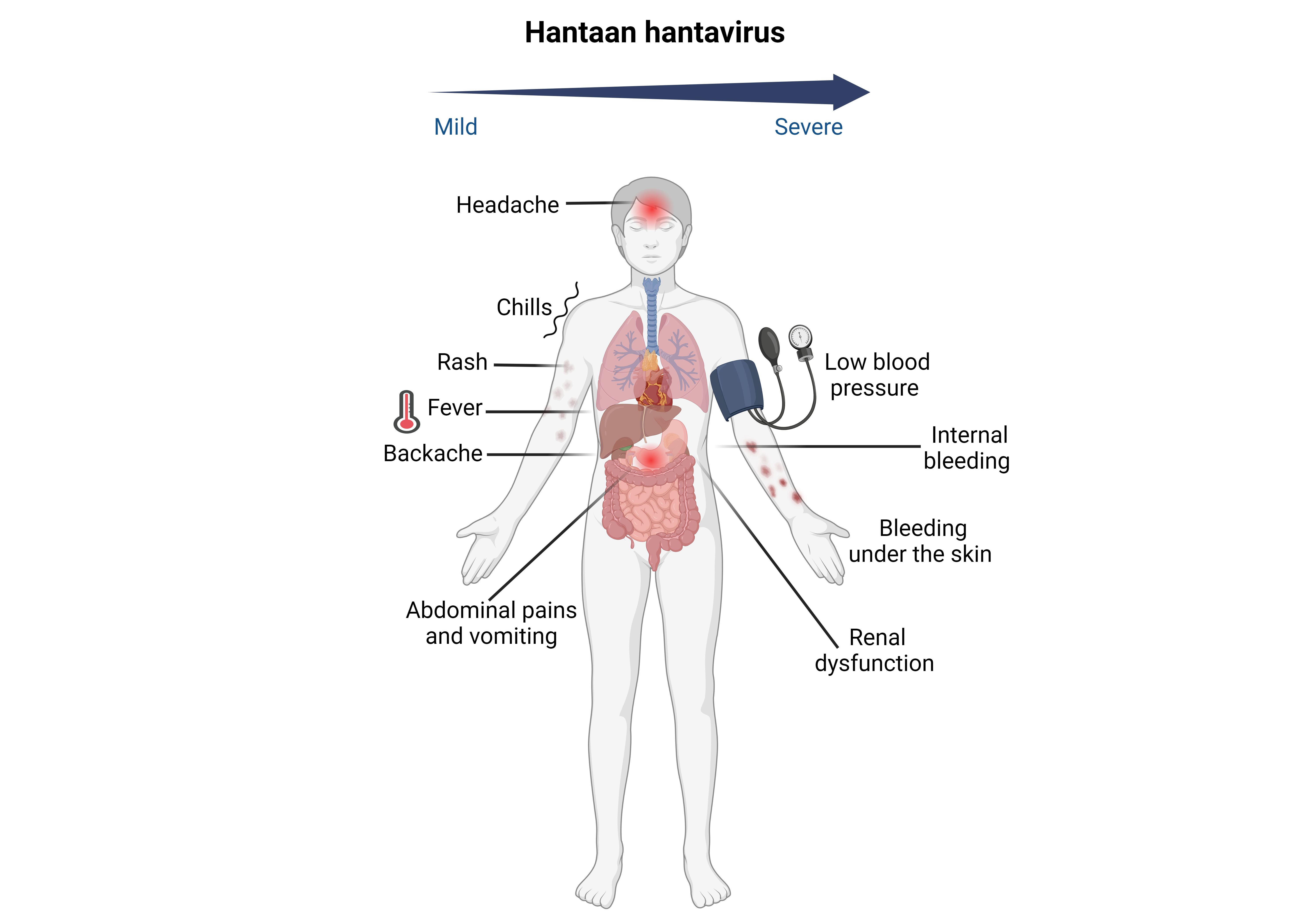
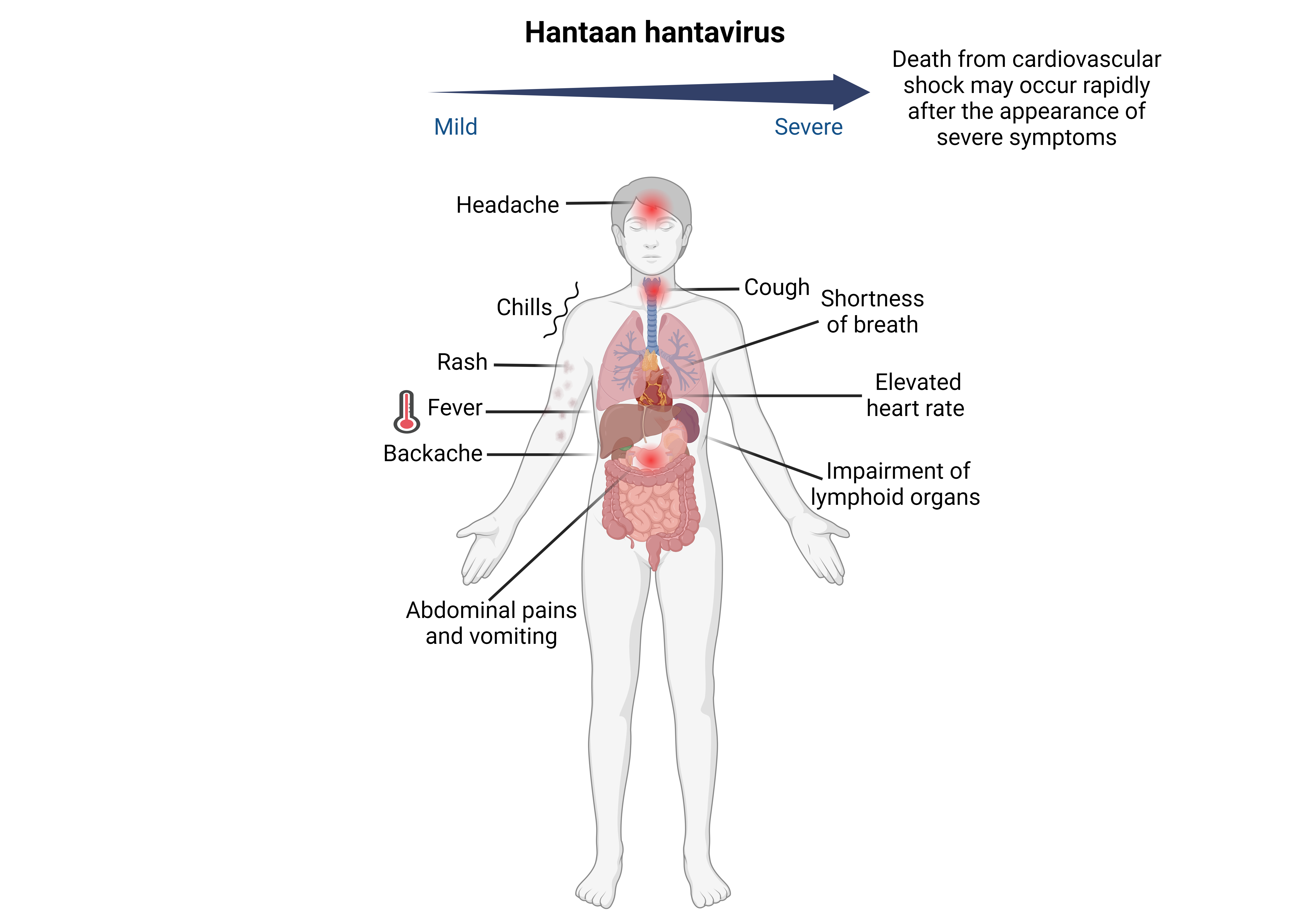
In 1976, the first pathogenic hantavirus, the Hantaan orthohantavirus, was isolated from rodents near the Hantan River in South Korea.
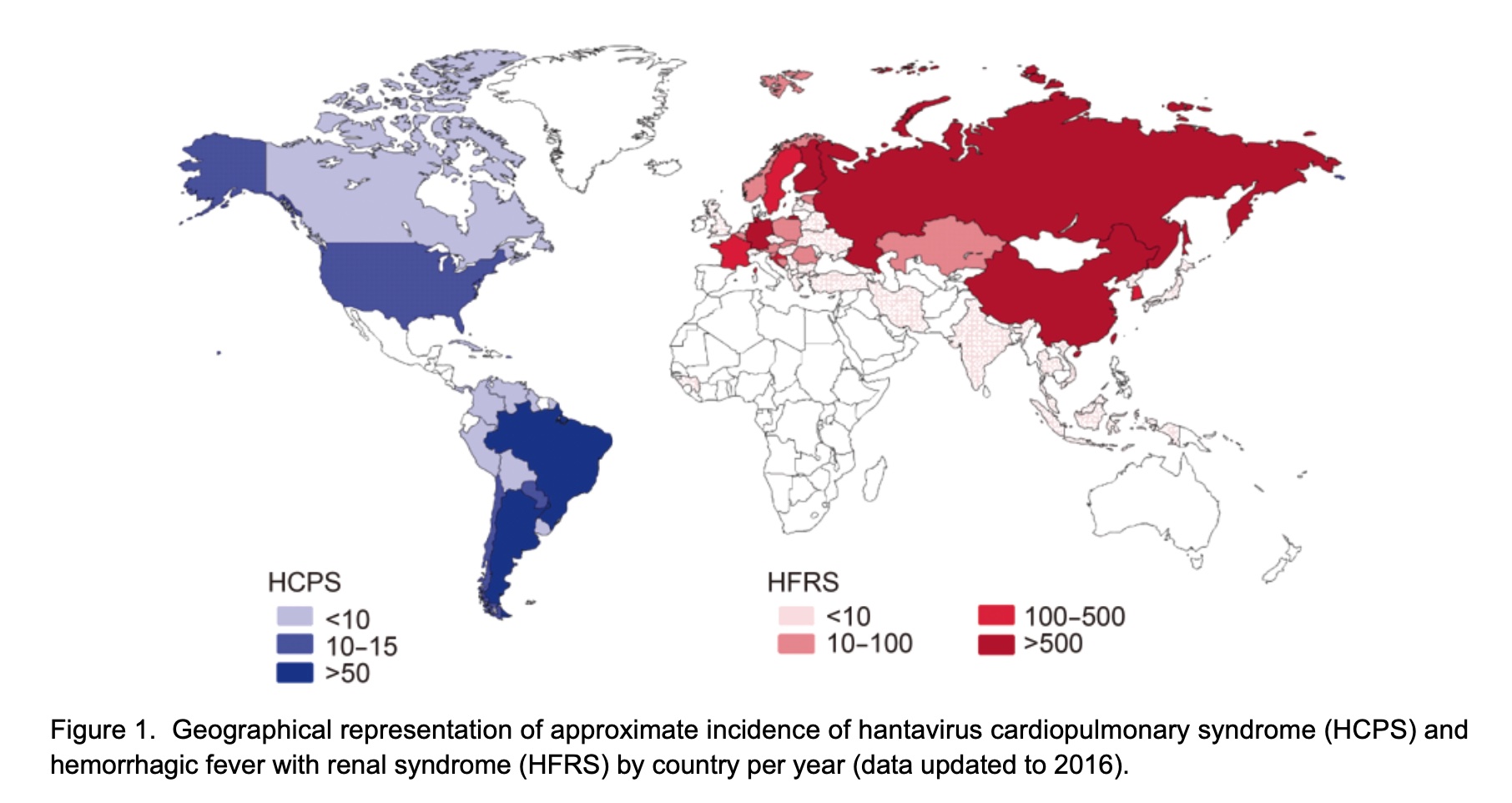
It is the causative agent of Korean hemorrhagic fever in humans. Regions especially affected by HFRS include China, the Korean Peninsula and Russia.
The toolbox for this virus is currently in development. Please contact us via info@virusbankplatform.be for more information.
![]()
Andes orthohantavirus was first identified when outbreaks of this new infection spread throughout Chile and Argentina. It is named for the Andes mountains of Chile and Argentina, where it was first discovered.
In 1995, it was finally characterized in Argentina on the basis of specimens from a patient who had died from HPS complications, a severe consequence of infection from Andes viruses.
As an emerging virus, it is more lethal than that of some of the other hantaviruses having a mortality rate between 40% and 50% in South America.
By far, it has been responsible for the most recorded cases of HPS in Argentina, Chile, and Uruguay combined and contributes to a large number of kidney failure cases.
The toolbox for this virus is currently in development. Please contact us via info@virusbankplatform.be for more information.
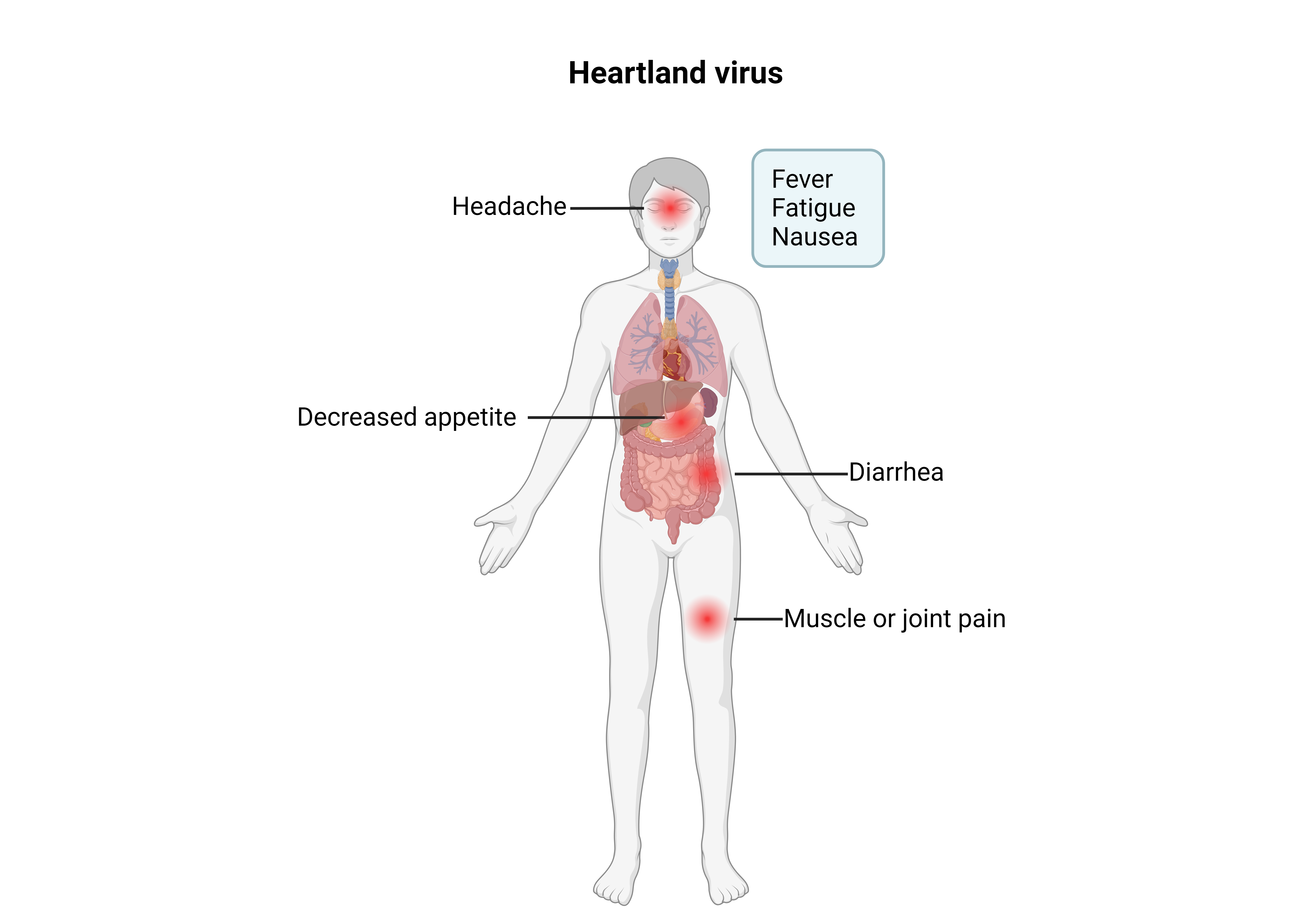
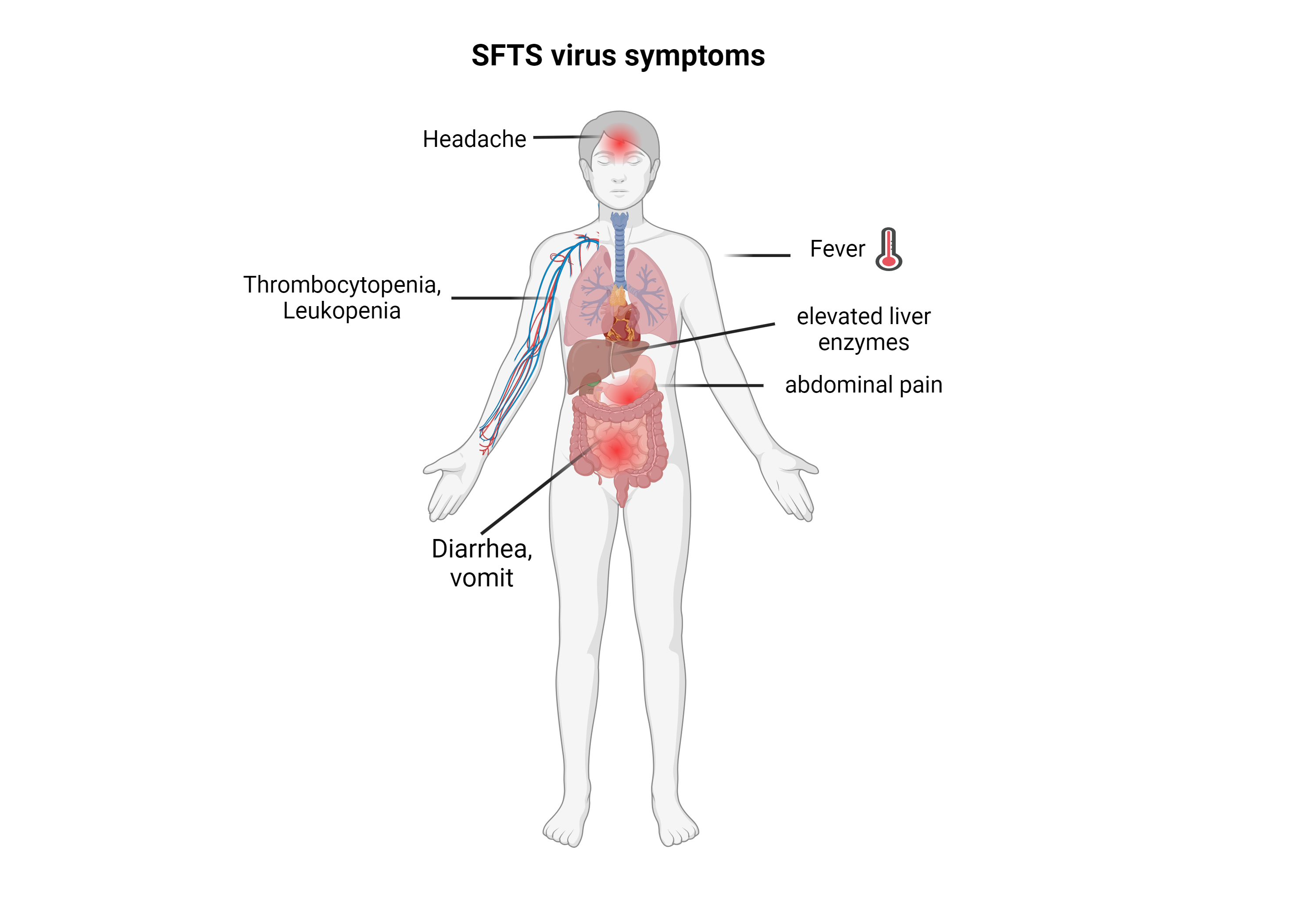
Some people also have lower than normal counts of white blood cells, also called leukopenia and thromobocytopenia.
![]()
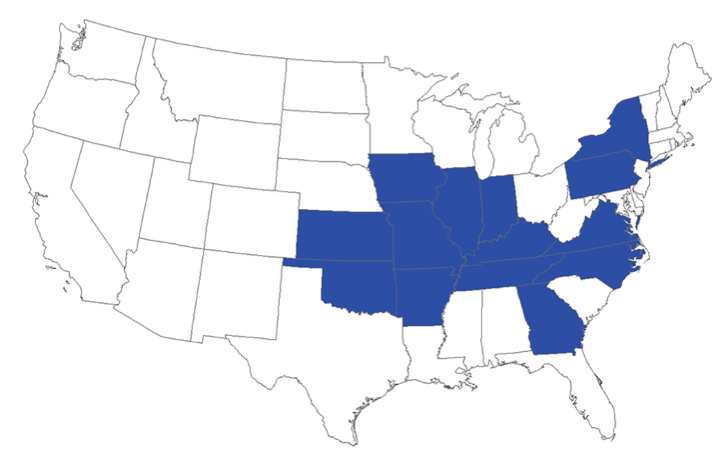
As of November 2022, more than 60 cases of Heartland virus disease have been reported from states in the Midwestern, Northeastern, and Southern United States.
Most people diagnosed with the disease became sick from May through September.
The toolbox for this virus is currently in development. Please contact us via info@virusbankplatform.be for more information.
![]()
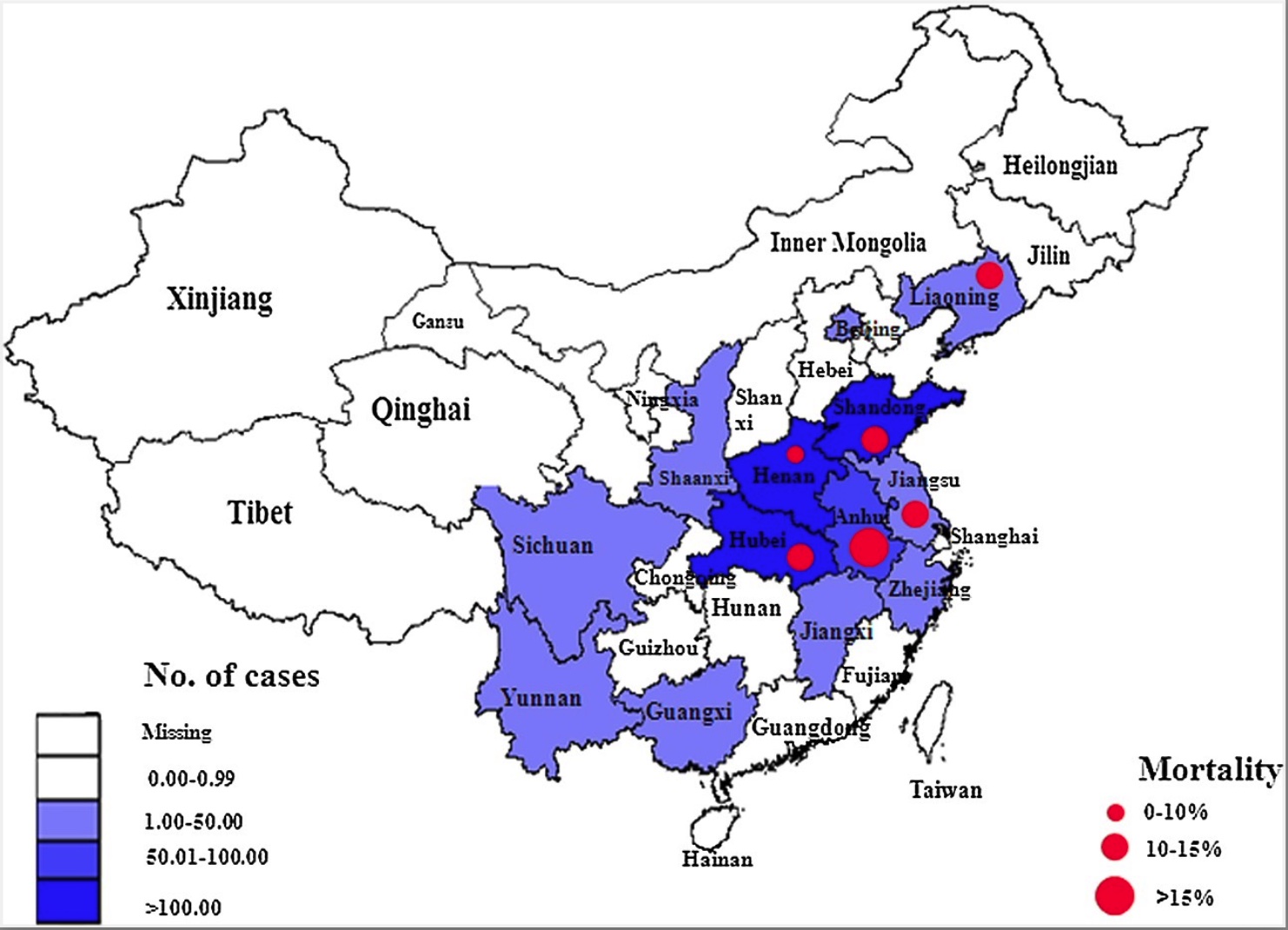
SFTS is an emerging infectious disease that was first described in northeast and central China 2009 and now has also been discovered in Japan, South Korea, Vietnam and Taiwan in 2015.
Another outbreak occurred in East China in the early half of 2020.
SFTS has a fatality rate of 12% and as high as over 30% in some areas.
The toolbox for this virus is currently in development. Please contact us via info@virusbankplatform.be for more information.
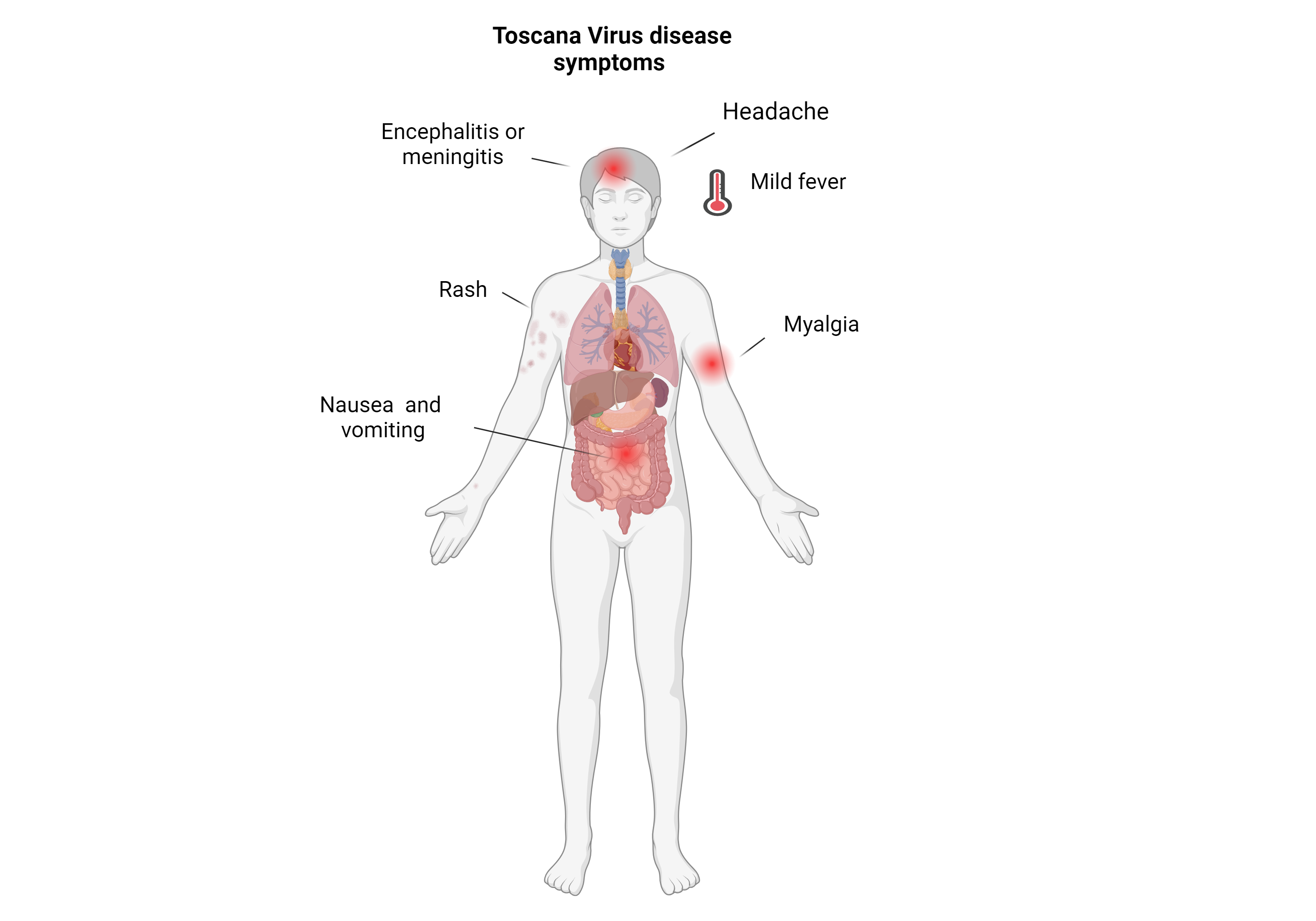
Most people infected are asymptomatic .
In serious cases that go undiagnosed, acute meningitis, meningoencephalitis and encephalitis may occur. In rare instance, fatal encephalitis has been reported.
![]()
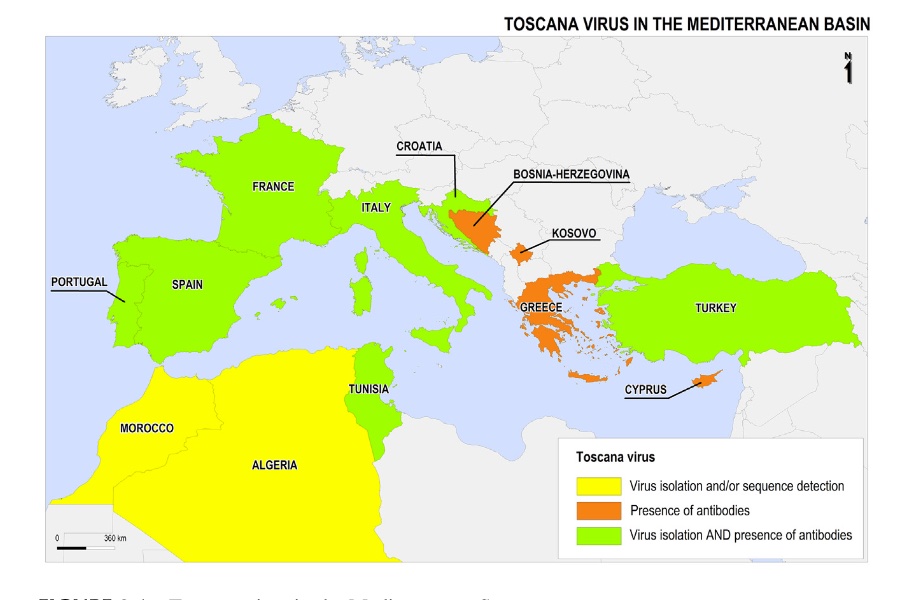
Toscana virus was first isolated in 1971 from sand flies collected in the Tuscany region of Italy and first evidence for its propensity to cause human disease was reported in 1983.
This virus is a leading cause of acute meningitis between May and October in Central Italy and in other northern Mediterranean countries (Croatia, France, Greece, Portugal and Spain) as well as several of the eastern Mediterranean countries (Cyprus and Turkey).
It is among the 3 most prevalent viruses associated with meningitis during the warm seasons: the other two are enteroviruses and herpesviruses.
The toolbox for this virus is currently in development. Please contact us via info@virusbankplatform.be for more information.
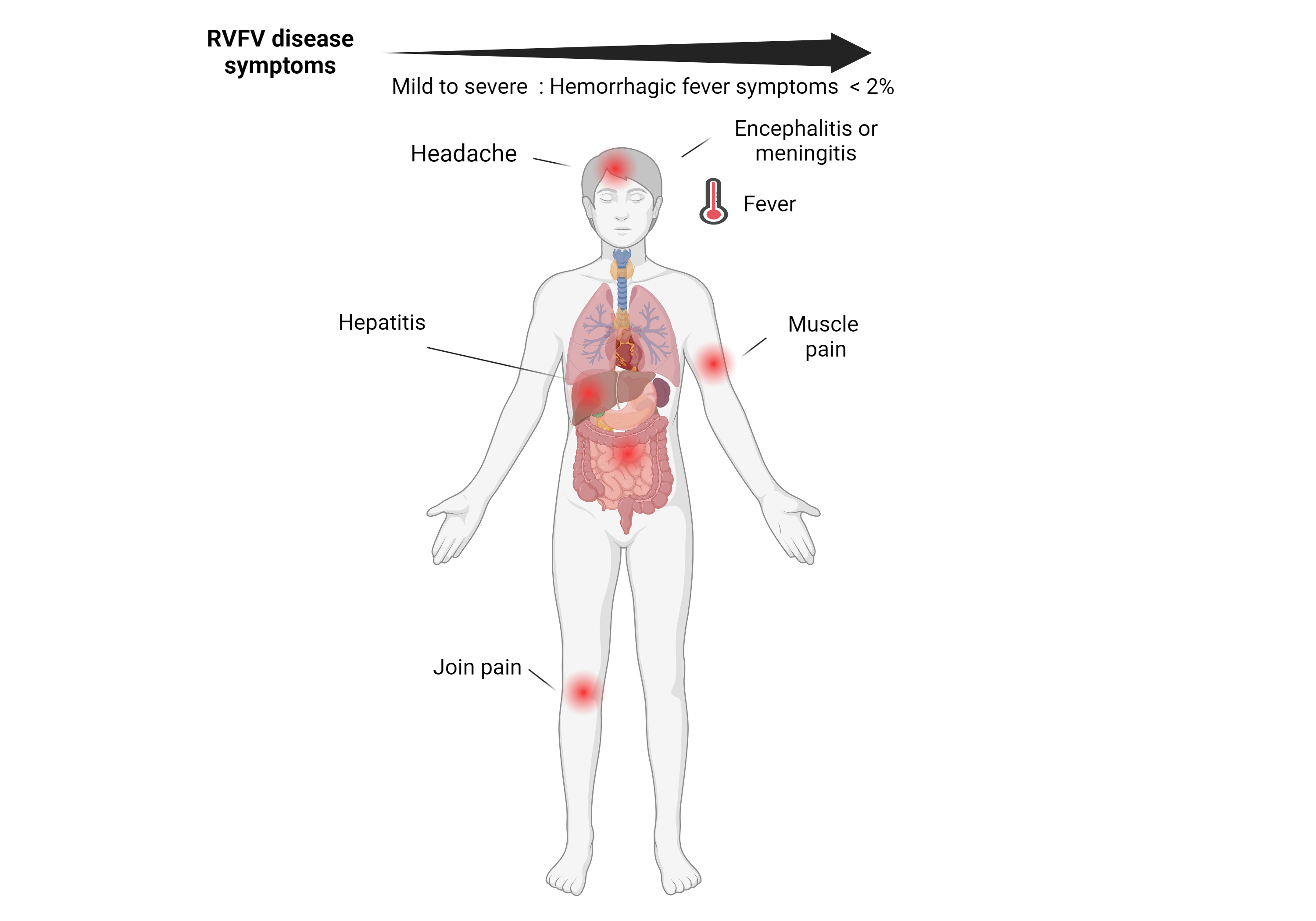
Patient are asymptomatic or only a mild illness with fever, headache, muscle pains, and liver abnormalities.
< 2% of cases, the illness can progress to hemorrhagic fever syndrome, meningoencephalitis or affect the eye.
People recover within 2-7 days after onset of symptoms.
1% of people with the disease die of it. Those who have bleeding have a chance of death as high as 50%.
![]()
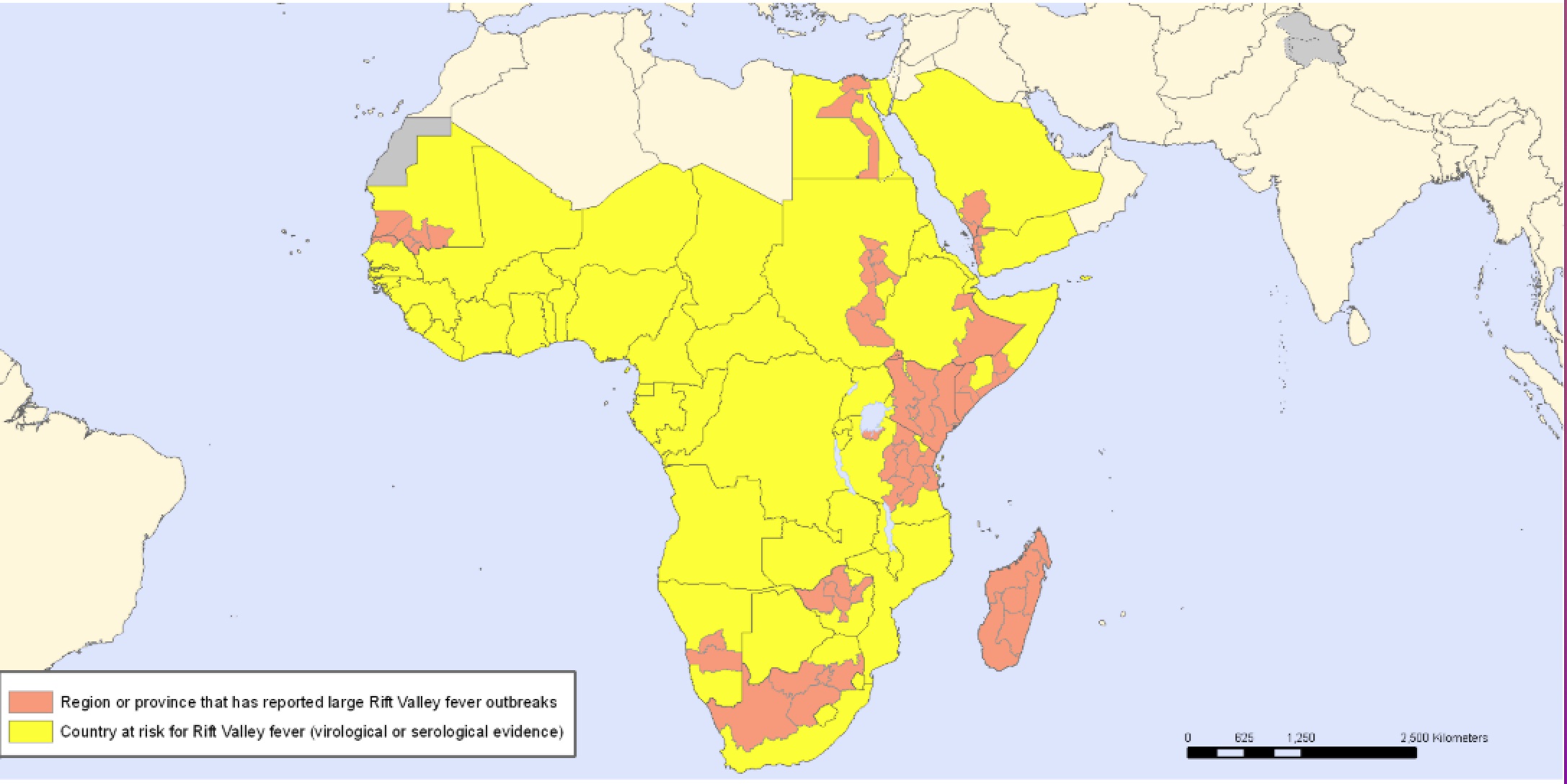
Rift Valley fever virus (RVFV) was originally discovered as the causative agent of an outbreak of ‘enzootic hepatitis’ in 1930 near Lake Naivasha in the Rift Valley of Kenya.
The virus is now endemic throughout multiple African countries and the Arabian Peninsula.
Outbreaks of the disease have only occurred in Africa and Arabia. Outbreaks usually occur during periods of increased rain which increase the number of mosquitoes.
The toolbox for this virus is currently in development. Please contact us via info@virusbankplatform.be for more information.
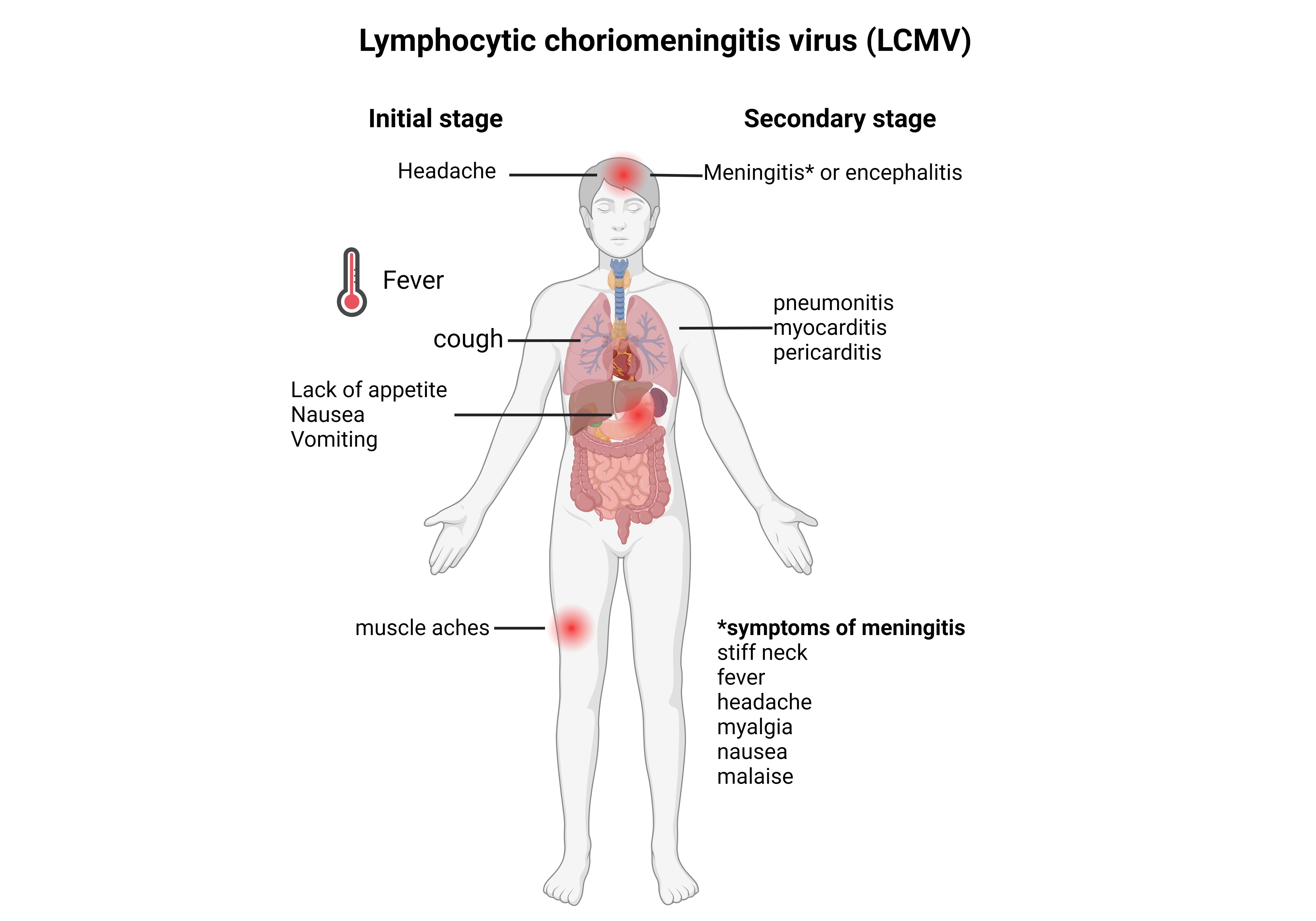
The onset of the second phase occurs several days after recovery, and consists of symptoms of meningitis or encephalitis.
The entire illness usually lasts 1 to 3 weeks, nonetheless, temporary or permanent neurological damage is possible in all central nervous system infections, especially in cases of meningoencephalitis.
Chronic infections have not been reported in humans and deaths rarely occur.
![]()
Lymphocytic choriomeningitis mammarenavirus (LCMV), was isolated in 1933 by Charles Armstrong during a study of an epidemic in St. Louis. Although not the cause of the outbreak, LCMV was found to be a cause of nonbacterial or aseptic meningitis.
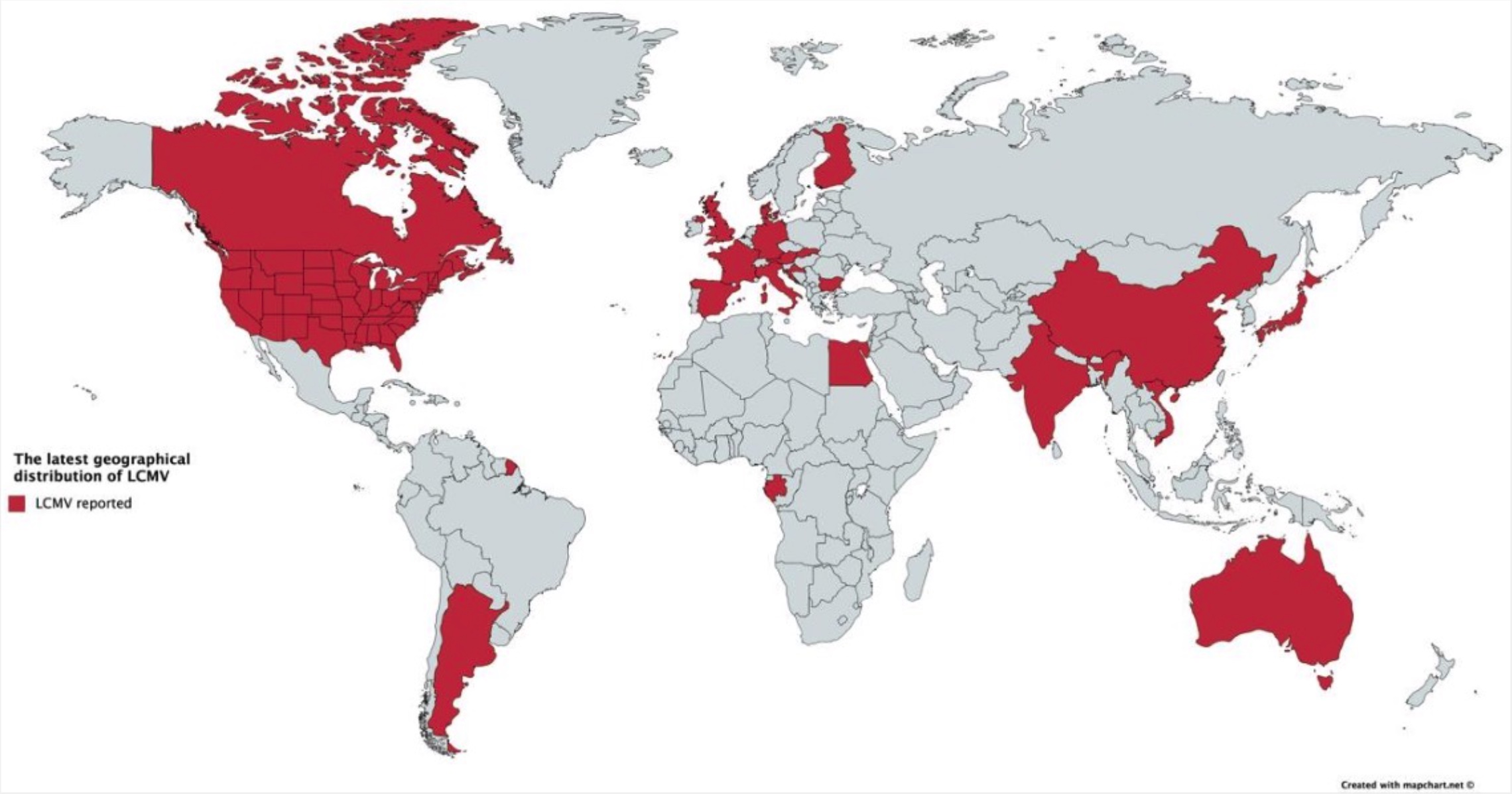
Cases of lymphocytic choriomeningitis have been reported in North and South America, Europe, Australia, and Japan, particularly during the 1900s.
LCMV occurs now worldwide and its natural host, the rodent, has become established on all continents, except Antarctica.
Studies have indicated that human infection of the virus occurs primarily during the fall and winter months, presumably due to the movement of mice indoors.
The toolbox for this virus is currently in development. Please contact us via info@virusbankplatform.be for more information.
![]()
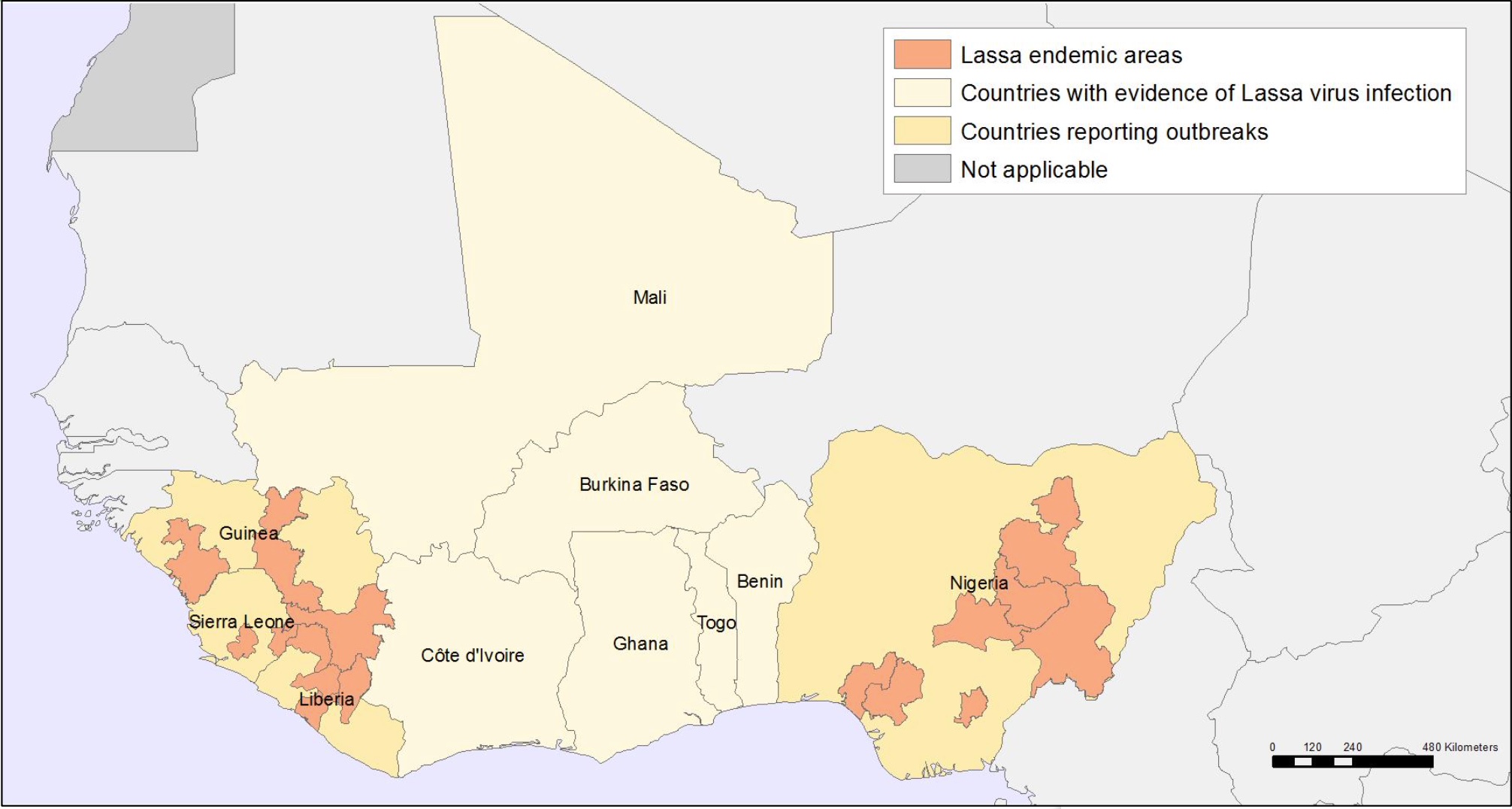
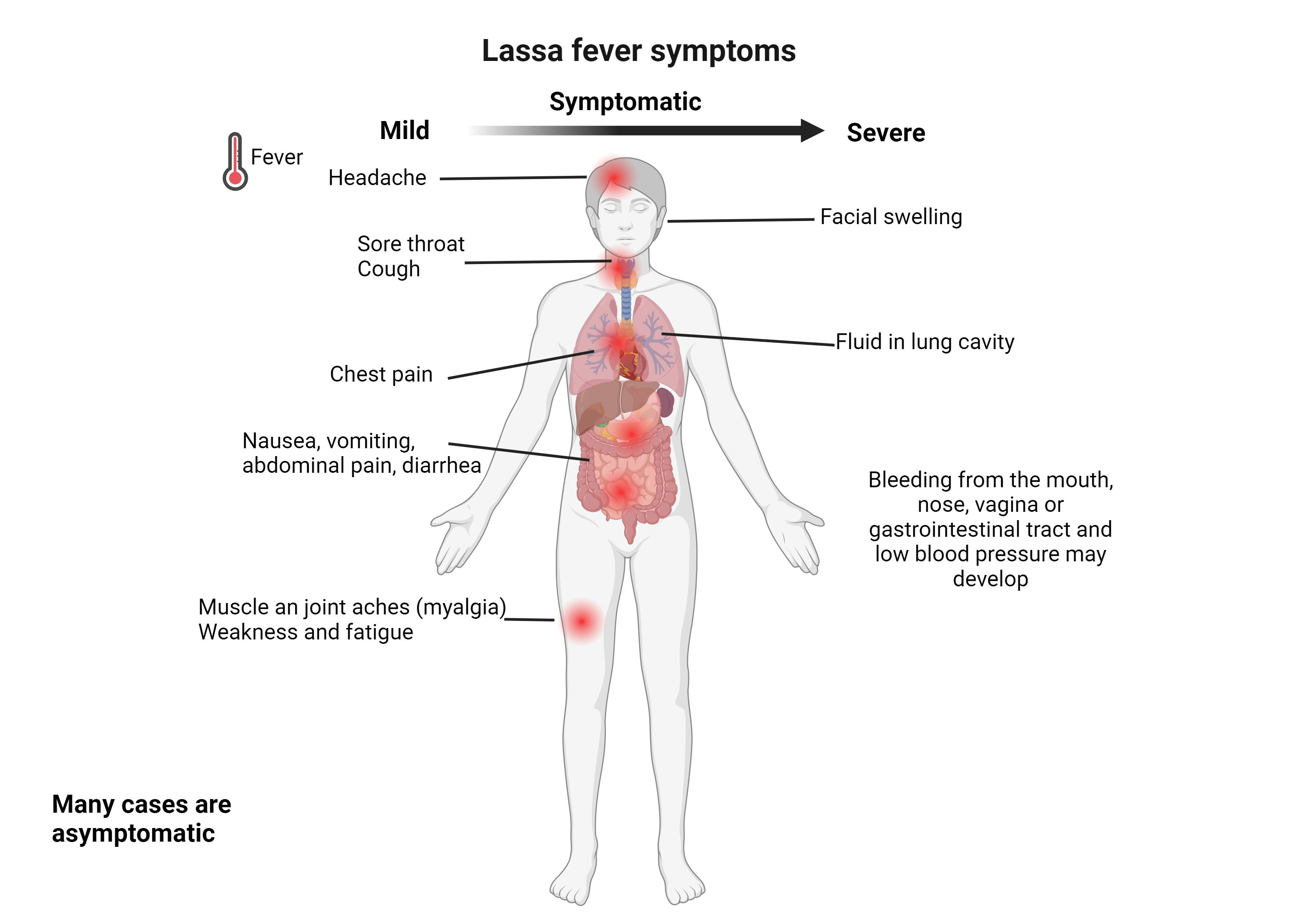
The virus was first described in 1969 from a case in the town of Lassa, in Borno State, Nigeria.
Lassa fever is relatively common in West Africa including the countries of Nigeria, Liberia, Sierra Leone, Guinea, and Ghana.
There are about 300,000 to 500,000 cases which result in 5,000 deaths a year.
Approximately 15%-20% of those who have required hospitalization for Lassa fever die.
The risk of death is greater in those who are pregnant.
The toolbox for this virus is currently in development. Please contact us via info@virusbankplatform.be for more information.
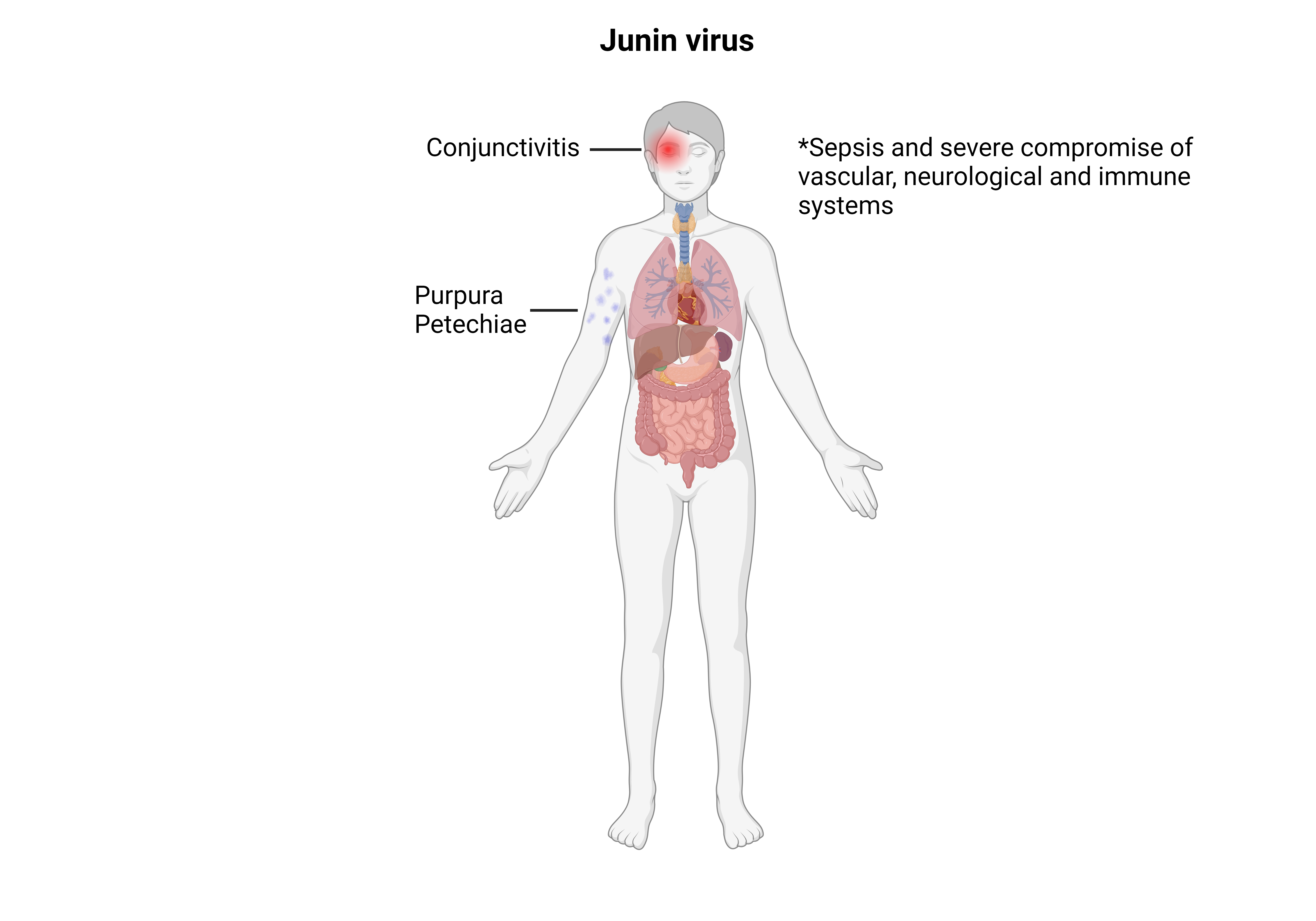
Junin virus infection has a mortality rate between 20 and 30%.
![]()
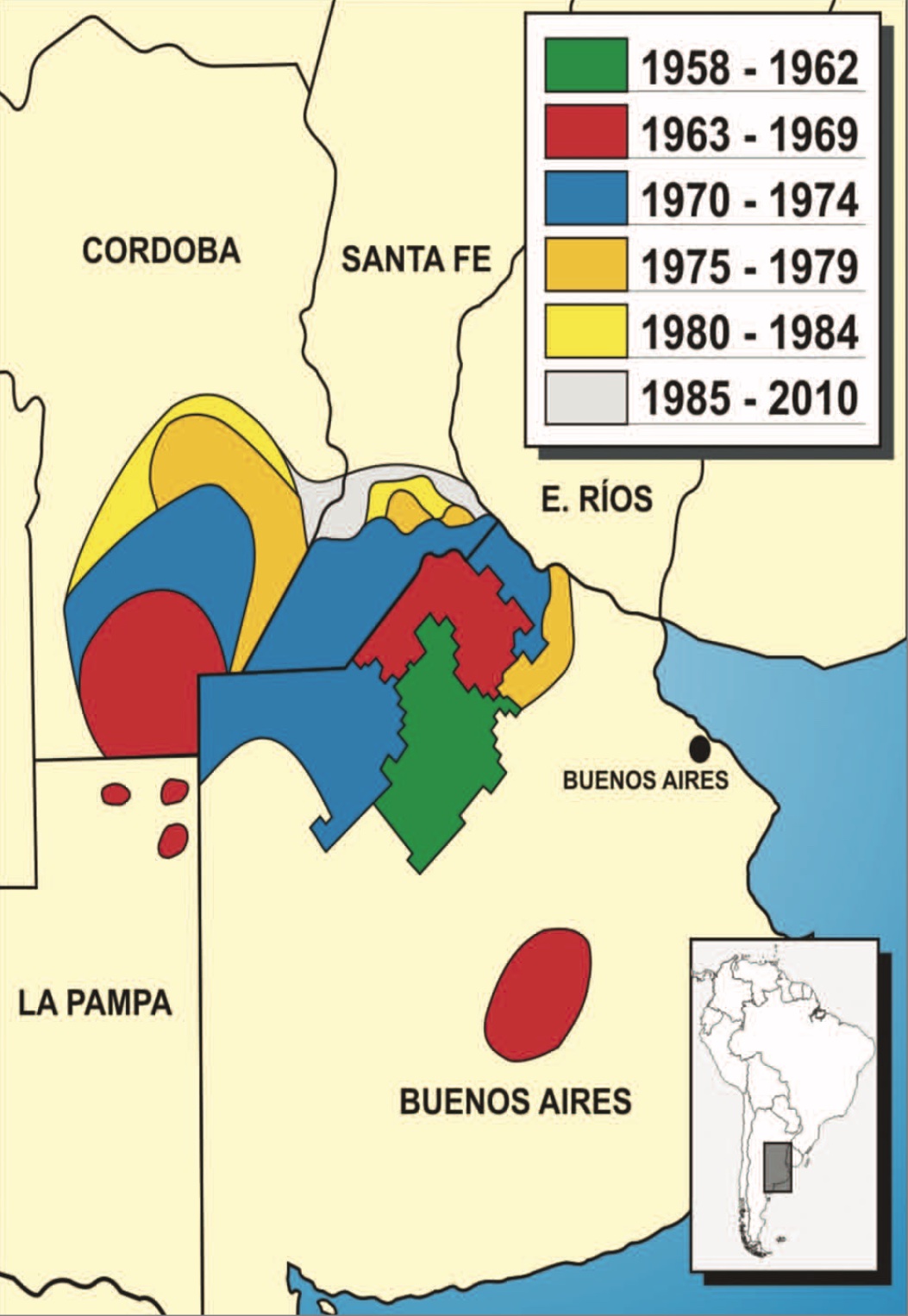
Argentinian mammarenavirus, better known as the Junin virus or Junín virus (JUNV), is an arenavirus that causes Argentine hemorrhagic fever (AHF).
The virus took its original name from the city of Junín, around which the first cases of infection were reported, in 1958.
Since the discovery of Argentinian mammarenavirus in 1958, the geographical distribution of the pathogen, although still confined to Argentina, has expanded. At the time of discovery, Argentinian mammarenavirus was confined to an area of around 15,000 km2. At the beginning of 2000, the region with reported cases grew to around 150,000 km2.
The toolbox for this virus is currently in development. Please contact us via info@virusbankplatform.be for more information.